In 2002, across London, the UK’s largest study on young people from ethnic minority backgrounds began its decade long research. Its findings uncovered a potentially disturbing relationship between exposure to racism and teenage smoking.
***
It is no surprise that very few studies have investigated the impact economic adversity and psychosocial factors have on young people of colour. This study, conducted by Kings College London, aimed to uncover any possible links between exposure to racism and the smoking of tobacco, in the ethnically diverse population of young people in London.
The Race Disparity Audit, released late last year, was the government’s lack lustre response to the “burning injustices” referenced in Theresa May’s party election speech in 2016. Young people from ethnically diverse backgrounds are more likely to experience economic hardship than their white British peers; in the wake of the EU referendum there has been a marked increase in reported hate crime that is either religiously and/or racially motivated. The reality of racism began long before the soundbites of Mrs May, yet what we have neglected to discuss, amongst all the reports and audits, is the life-long impact such injustices can have on the physical and mental health of individuals.
At the start of this study, over 6,000 children, aged between 11-13 years were classed within an ethnic group: White British, Indian, Pakistani or Bangladeshi, Black African, Black Caribbean, and others. Those from ethnic minority groups, compared to their White British peers, were less likely to have smoked, yet more likely to report experiences of racism.
In this study, racism and discrimination were identified by a positive answer to these two questions: “Has anyone made you feel bad or hassled you because of your race, skin colour, or where you were born?” and “Has anyone made you feel bad or hassled you because of your religion?”
The study also found that:
- At 14-16 years, the proportion of those who had initiated smoking increased across all ethnic minority groups, but was still lower than white British figures
- There is a significant increase of Black African females reporting racism at ages 14-16 compared to just two years prior at the start of the study
- A larger proportion of ethnic minority groups expressed a controlling relationship with their parents
- Less than 20% of ethnic minority groups have no religious affiliation
- At 21-23 years, ethnic minorities were still more likely to report racism and attend a place of worship, but less likely to smoke
- The relationship between racism and smoking does not vary gender or ethnicity
Whilst the study cannot demonstrate causation between experiencing racism and smoking behaviour, a correlation has been exposed: racism shows some association to smoking behaviour.
The findings of the study beg the question, is racism a negative health determinant? Professor Seeromanie Harding, lead investigator of the study, said: “An important point here is that racism affects both physical and mental health outcomes. Addressing racism is an important public health priority for young people.”
Exposure to racism triggers a physiological stress response. Racism is often discussed as a social construct, manifested in interpersonal experiences, or as a part of an institution designed to discriminate based on race or religion. This study starts a whole new conversation on whether we now need to treat racism as a public health concern.
“…the increase in smoking initiation among ethnic minority groups paints a disappointing picture of the truth of health inequalities”
We know that responses to stress may not lead to the healthiest life choices, whether that is drinking, smoking or drug use. But if we treat racism like any other external stress-inducing factor, should we not be more concerned by the increasing likelihood of our youth being drawn to unhealthy coping mechanisms?
Those who reported racism between 11-13 and 14-16 years were 80% more likely to start smoking by the age of 16. That is a generation of ethnically diverse young people who are now more at risk of developing smoking-related diseases that may already be disproportionately high in their ethnic populations.
Now more than ever are we aware of the strain on our health services. We are inundated by stories of the NHS failing to meet targets, hospitals being threatened with closure and the numbers of nurses and doctors falling. And whilst the UK has seen a significant decrease in smoking amongst adolescents, the increase in smoking initiation among ethnic minority groups paints a disappointing picture of the truth of health inequalities.
“It takes a village to raise a child” goes the ancient African proverb. And so, this study also aimed to investigate if positive relationships, with parents, peers and religion, could act as a buffer for the negative impact racism has on smoking behaviour.
Through the analysis of qualitative and quantitative measures, the study found that individuals from all ethnic groups that expressed positive family relationships were less likely to start smoking. Positive parenting lent itself to nurturing self-esteem as well as learning “positive coping strategies”. Religious involvement is also attributed to instilling morals and values that contradict negative health behaviours. Adolescents who had experienced racism, but did not attend a place of worship were found more likely to smoke than those who do.
“We now have a scientific reference point for discussions on the impact racism has on ethnic minority groups”
Whilst there are several factors that contribute to a person taking up smoking, the wider implications of a study such as this are incredible. We now have a scientific reference point for discussions on the impact racism has on ethnic minority groups. However, like any scientific discovery, there are limitations to its findings.
In the UK, 20% of the population belong to ethnic minority groups, whilst in London that figure is 55%. London is a beautifully ethnically diverse city, and the experiences of ethnic minorities cannot be generalised for all parts of the country. It must also be considered that cultural or religious disapproval of risk behaviours, such as smoking, may be strongest for girls than boys, as in some cultures females are subject to more scrutiny.
Research by think tank The Runnymede Trust and The Women’s Budget Group report that black and ethnic minority women sufferer the hardest hits from government cuts, and as we enter another year or austerity under a Tory government hopes of economic prosperity for the most disadvantaged are scarce.
With racism-related stress now an incontestable determining factor in the physical and mental health of an individual, and hate crimes and discrimination on the rise in a post-Brexit Britain, it’s clear that the well-being of Britain’s disenfranchised are not a priority for the current government.
If we, as a nation of people from all ethnicities and religions, continue to avoid conversations on the impact racism can have on the physical and mental health of young people, we only risk widening the gap in health inequalities.

Britain’s policing was built on racism. Abolition is unavoidable
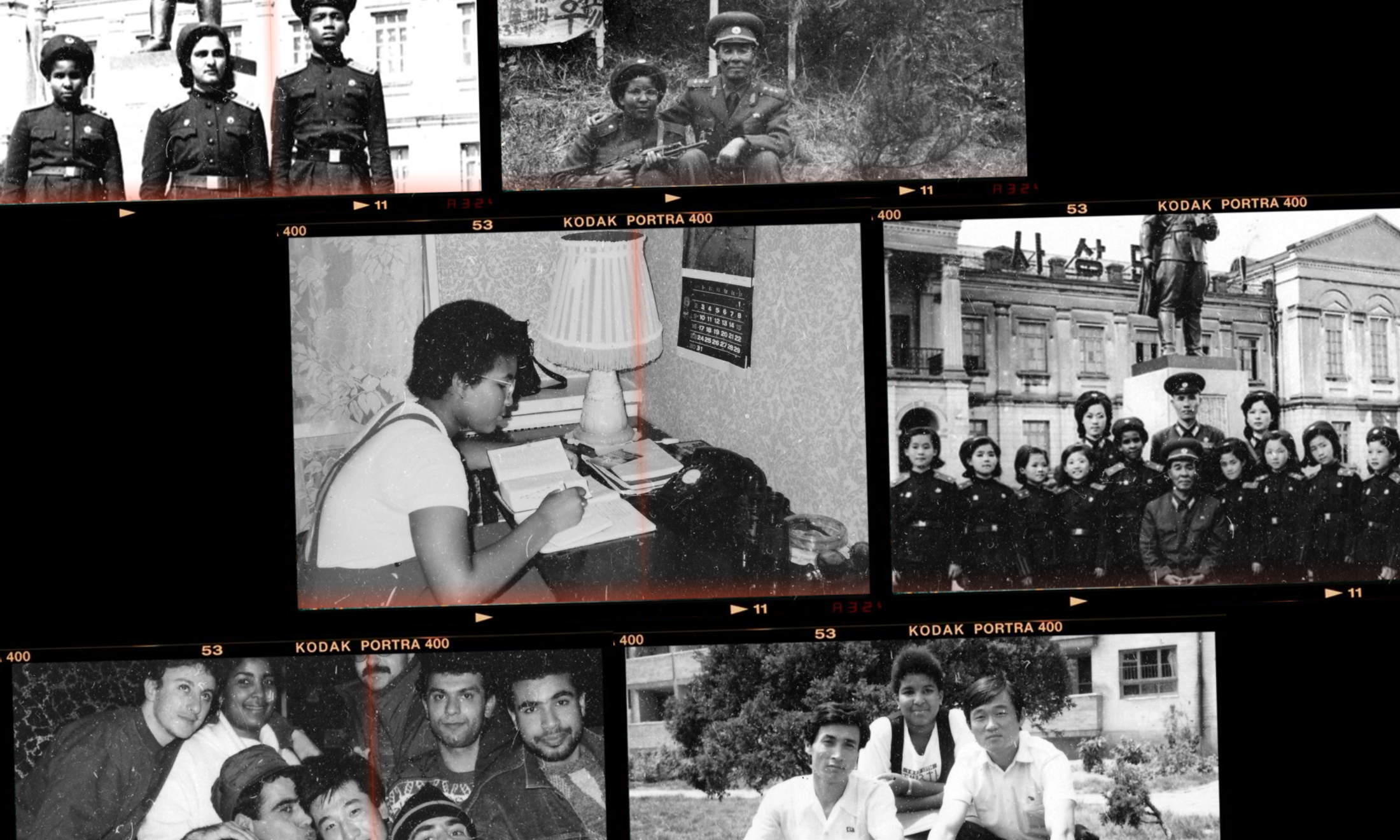
Growing up as a Black girl from Pyongyang

From #SayHerName to ‘woke’, is the language of Black liberation being looted?

Let’s stop comparing celebrity pregnancies, please